Cancer Research: Oncolytic Viruses / Rigvir
STEP ONE
Be informed. Read information below.
STEP TWO
Schedule consultation with R. Douglas Wichman, MD.
STEP THREE
Submit "New Patient Form", current labwork, & imaging results prior to consultation.
STEP FOUR
Establish if you are a candidate for this therapy
in accordance with the Georgia
"Access to Medical Treatment Act".
----------------------------------------------------------------------------------------------------------------------------------------------------------
*** SPECIAL NOTE FROM DR. WICHMAN ***
The following excellent article was reproduced from Melanoma Research at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4560272/:
Adapted ECHO-7 virus Rigvir immunotherapy (oncolytic virotherapy) prolongs survival in melanoma patients after surgical excision of the tumour in a retrospective study
 d Björn Jonsson,e,✠ Dite Venskus,dand Aina Mucenieced,✠
d Björn Jonsson,e,✠ Dite Venskus,dand Aina Mucenieced,✠Introduction
Melanoma is one of the fastest-growing cancers and has the highest mortality rate of skin cancers 1–3. More than half of melanoma patients experience progression of the disease within 3 years of diagnosis 4,5. Current clinical practice guidelines for stage I–II melanoma provide few, if any, recommendations for treatment 6–9. The oncolytic property of viruses has been observed for over a century and is presently being studied intensively 10–16. An oncolytic, nonpathogenic ECHO-7 virus, adapted and selected for melanoma that has not been genetically modified (Rigvir), was approved and registered in 2004 in Latvia for melanoma therapy 17–27. The effect of viruses on cancers, including melanoma, has been tested in clinical trials; however, the effectiveness of an approved and marketed virus has not yet been shown in a clinical setting 12,14,16.
In oncolytic virotherapy, Rigvir is a first-in-class. At a later time, a genetically modified adenovirus was approved for head and neck cancer 28,29. Melanoma is staged with substages from 0 to IV by measuring the thickness of the tumour according to Breslow, by assessment of ulceration, mitotic rate and metastases and by collecting pathologic information on regional lymph nodes 30,31. On the basis of the stage of the disease, treatment is currently performed according to published guidelines 4,6–9.
The aim of the present study is to test the effectiveness of Rigvir in a retrospective study in substage IB, IIA, IIB and IIC melanoma patients on time to progression and overall survival.
Methods
Retrospective clinical study patients
White patients (N=79) who had undergone surgical excision of melanoma and diagnosis verified histologically during the 4 years between January 2008 and December 2011 were included in this study. All patients were free of disease after surgery and were classified into substages IB, IIA, IIB and IIC according to the American Joint Committee on Cancer 30,31. For disease progression, all were followed for a minimum of 3 months until January 2014. The overall survival was checked on 5 June 2014 and considered to reflect the status by 27 May 2014. The detailed study population characteristics of this retrospective study are shown in Table Table11.
Current guidelines for melanoma advise no treatment postsurgery for patients who are classified into substages IB and IIA. Patients in substages IIB and IIC are provided three options: participation in a clinical trial, observation and interferon 7,8. In the absence of strict guidelines, treatment with Rigvir was offered. Thus, 52 study participants received Rigvir and 27 were observed according to the guidelines. The patients who had been treated with interferon were excluded from the present analysis as, in the registry, they were too few to allow for any comparison.
As a part of the safety assessment, serum clinical chemistry parameters were recorded.
The patients in this study were treated in the Latvian Oncology Center of Riga Eastern Clinical University Hospital, the Latvian Virotherapy Center in Riga and the Oncology Clinic of Piejūras Hospital in Liepāja, Latvia.
The study was approved by the respective ethics committee.
Rigvir characteristics
Rigvir is a 2 ml frozen solution of an adapted and selected ECHO-7 virus strain, Picornaviridae family, Enterovirus genus, Enteric Cytopathic Human Orphan (ECHO) type 7, group IV, positive-sense single-stranded RNA virus produced under GMP. The titre is not less than 106 TCID50/ml in sodium chloride for injection.
Method of Rigvir administration
Treatment was started after surgical excision of the primary melanoma tumour when the wound had healed. First, Rigvir (2 ml) was administered intramuscularly regionally for 3 consecutive days. After about 4 weeks, administration was repeated for three consecutive days and repeated about 4 weeks later. Subsequently, a single administration of Rigvir (2 ml, intramuscularly) was performed at monthly intervals during the first year, at 6-week intervals during the first half of the second year, at 2-month intervals during the second half of the second year and at 3-month intervals in the third year. Rigvir is not to be used during an acute infection.
Statistical analysis
Statistical analysis of the data was carried out using the SPSS statistical software, V.20 (SPSS Inc., Chicago, Illinois, USA). Mann–Whitney U-test and Wilcoxon tests (for continuous variables), Fisher’s exact test and the χ2-test (for categorical variables) were used to test differences between and within groups. Cox proportional hazard survival regression analysis was carried out, which is the most commonly used multivariate model in survival analysis. Thus, any difference between the groups, for example, in age, has been taken into account in the Cox analysis. (This is in contrast to Kaplan–Meier analysis, which is a bivariate analysis that only takes into account one predictor at a time). Hazard ratios (HRs) and 95% confidence intervals were calculated using bivariate and multivariate Cox regression analysis on survival. Endpoints were occurrence of metastases or disease recurrence for time to progression, and death from any cause for analysis of overall survival. Predictors (covariates) used in regression analysis were tumour stages, treatment (Rigvir, observation), sex and age. A P value less than 0.05 from a two-sided test was established to indicate statistical significance.
Results
Effectiveness in patients: time to progression
Melanoma patients of substages IB, IIA, IIB and IIC were studied according to the postsurgery management that they had received. One group was treated with Rigvir and the other was managed according to current guidelines by observation (the control group is called ‘observation’) 6–9. The follow-up period was not statistically different between both treatment groups (Table (Table11).
Patients who were free of melanoma after surgical excision and were treated with Rigvir appeared to remain disease free (free of metastases and/or recurrence) for a longer period of time compared with a similar group of patients who did not receive Rigvir. The difference between the treatment groups did not, however, reach statistical significance (Table (Table22).
Effectiveness in patients: overall survival
The survival of patients who were treated with Rigvir was significantly (P<0.05) longer compared with a similar group of patients who did not receive Rigvir (Fig. (Fig.11 and Table Table3).3). The difference between both treatment groups was statistically significant on analysing all four substages together (IB, IIA, IIB, IIC) (Table (Table3)3) and on analysing stage II together (substages IIA, IIB, IIC). Adjusting for patient age, sex and substage of disease, the HR was calculated in multivariate Cox regression analysis. The HR for patients treated according to current guidelines by observation versus treated with Rigvir was 6.27 (P<0.005) for all patients, 4.39 (P<0.032) for substage IIA–IIC patients and 6.57 (P<0.014) for substage IIB–IIC patients (Fig. (Fig.1).1). This indicates that the patients who were treated with Rigvir had a 4.39–6.57-fold lower mortality than those treated using current guidelines by observation.

Safety assessment
In the previous clinical studies, a few side effects were reported, for example subfebrile temperature (37.5°C for a couple of days), pain in the tumour area, sleepiness and diarrhoea. In this retrospective study, however, there was no record of any untoward side effect from Rigvir treatment or its discontinuation.
Serum clinical chemistry parameters were recorded and graded according to NCI CTCAE 32 (Table (Table4).4). In the observation group, grade 1–3 values were obtained. All grade 3 samples were from two patients obtained within the last few months of life. In one of these patients, progression of the disease was reported simultaneously. In contrast, in the Rigvir-treated patients, values above grade 2 were not observed.
Discussion
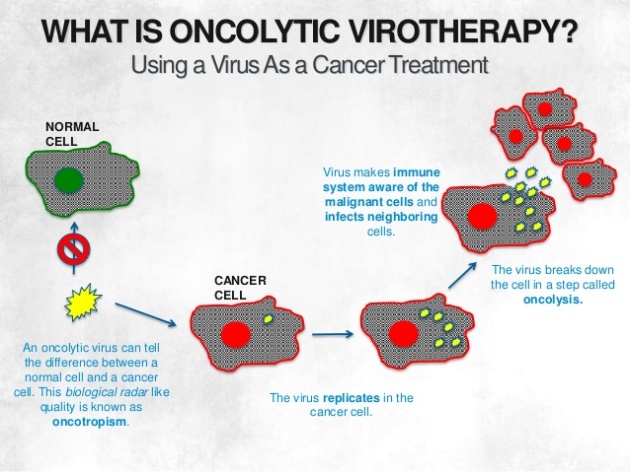
Oncolytic virotherapy is one of three forms of virotherapy (the other two being viral vectors for gene therapy and viral immunotherapy, respectively). Early observations of tumour regressions after virus infections have been published starting from the late 19th century (cf. 10–16). Recently, several oncolytic viruses have been tested clinically 33–35 and Science named cancer immunotherapy the breakthrough of the year of 2013 36. The melanoma adapted and selected ECHO-7 virus Rigvir is first-in-class in oncolytic virotherapy; it is approved as therapy for melanoma.
The present results show that in substage IB, IIA, IIB and IIC melanoma patients, Rigvir administration after surgery significantly (P<0.05) prolongs survival compared with patients who were managed according to current published guidelines 6–9. For the Rigvir-treated patients, the HR (risk of death) is 4.39–6.57-fold lower than for the control group treated according to current guidelines by observation. The HR was calculated in multivariate Cox regression analysis adjusting for patient age, sex and substage of disease.
In this study, there was no record of any untoward side effect from Rigvir treatment, which is in agreement with clinical studies using other oncolytic viruses 14,16,33,34,37. Moreover, no value higher than grade 2 was recorded in Rigvir-treated patients. This is in contrast to most other cancer therapies, where grades 3 and 4 are frequently observed (cf. 38).
Administration of virus induces the formation of neutralising antibodies that might potentially influence the efficiency of Rigvir. In previous studies, the titre of neutralising antibodies against ECHO-7 was determined in both healthy individuals and patients before administration of Rigvir. In 94 healthy adult participants tested, the titres were found to be low (1 : 20 to 1 : 62) 39,40. When tested in 155 adult cancer patients who had not been treated with Rigvir, neutralising antibodies against ECHO-7 were detected in ∼50% of the patients 41. In a local study of 472 individuals, the presence of ECHO-7 antibodies was shown to increase with age in children and level off to a plateau of around 75% in adults 42. To our knowledge, the prevalence of neutralising antibodies against the ECHO-7 virus in the general adult population has not been reported.
Rigvir is an immunomodulator that affects both the humoral, antibody-mediated, and the cellular immune systems 20–22. When virus adsorption and penetration to tumour tissue were measured, it was shown that they are not influenced by the presence of neutralising antibodies (titre 1 : 10) 43,44. Furthermore, in a preliminary study, the levels of neutralising antibodies to Rigvir during the first 18 months of treatment of melanoma patients did not appear to correlate with time to progression after 3 years of follow-up 40. In that study, the neutralising antibody titre was 1 : 10 before the start of treatment (N=34). After the first dose, the titre was 1 : 25 to 1 : 91 (determined 24–48 h after administration). A month later, before the second dose, the titre was 1 : 250 to 1 : 320 (N=30); after the second dose, it was 1 : 510 to 1 : 850. Two months later, before the third administration, the titre was 1 : 160 to 1 : 895 (N=26) and after the eighth dose, 18 months after the first dose, it was 1 : 280 to 1 : 1350 40.
Also, after intravenous administration, the correlation between antibody titres varies from one virus to another, and neutralising antibodies do not affect efficacy when local or regional administration is used 14,45,46.
An estimated 14.1 million new cancer cases were diagnosed worldwide in 2012, the latest available. The number is expected to increase to 24 million by 2035. About 232 000 patients are estimated to be diagnosed with melanoma in 2014 3. In the 20-year survival data analysis of the American Joint Committee on Cancer (cf. Figure 31.1 of 31), the majority of all melanoma patients belonged to stage I and stage II, 47 and 24%, respectively 31. However, at present, clinical practice guidelines suggest postsurgery therapy only for late-stage melanoma (radiation therapy and interferon α) 6–9.
Rigvir has also been used in other types of cancer. In vitro, it reduces the viability of melanoma, as well as pulmonary, gastric, pancreatic, bone, and breast cancer cell cultures 47,48. It is oncolytic in melanoma and rectum cancer patients 49,50 (26, p. 115) and has been shown to improve the 5-year survival in rectum cancer patients 24.
Taken together, the results suggest that a significant number of melanoma patients would benefit from prolonging the survival with Rigvir treatment. The results also show that this can be achieved without side effects. Results suggest that Rigvir could also be tested in the treatment of other types of cancer.
Conclusion
Rigvir is an oncolytic, nonpathogenic ECHO-7 virus that significantly prolongs survival in early-stage melanoma patients without any side effect.
Long-term treatment with the oncolytic ECHO-7 virus Rigvir of a melanoma stage IV M1c patient, a small cell lung cancer stage IIIA patient, and a histiocytic sarcoma stage IV patient-three case reports.
Abstract
Oncolytic virotherapy is a recent addition to cancer treatment. Here, we describe positive treatment outcomes in three patients using Rigvir virotherapy. One of the patients is diagnosed with melanoma stage IV M1c, one with small cell lung cancer stage IIIA, and one with histiocytic sarcoma stage IV. The diagnoses of all patients are verified by histology or cytology. All patients started Rigvir treatment within a few months after being diagnosed and are currently continuing Rigvir treatment. The degree of regression of the disease has been determined by computed tomography. Safety assessment of adverse events graded according to NCI CTCAE did not show any value above grade 1 during Rigvir(®) treatment. Using current standard treatments, the survival of patients with the present diagnoses is low. In contrast, the patients described here were diagnosed 3.5, 7.0, and 6.6 years ago, and their condition has improved and been stabile for over 1.5, 6.5, and 4 years, respectively. These observations suggest that virotherapy using Rigvir can successfully be used in long-term treatment of patients with melanoma stage IV M1c, small cell lung cancer stage IIIA, and histiocytic sarcoma stage IV and therefore could be included in prospective clinical studies.
© 2016 International Virotherapy Center. APMIS published by John Wiley & Sons Ltd.
- PMID:
- 27457663
- DOI:
- 10.1111/apm.12576
